Large clinical RCT trial finds no clear added benefit of catheter ablation for preventing recurrent stroke in patients with atrial fibrillation

Nationwide Japanese study provides first randomized evidence on combined ablation and DOAC therapy after strokeA nationwide clinical RCT trial led by Dr. Kazumi Kimura at Kumamoto University Hospital has found that adding catheter ablation to standard anticoagulant therapy did not significantly reduce the risk of recurrent stroke or major cardiovascular events in patients with atrial fibrillation who had recently experienced a stroke.
Atrial fibrillation is the most common type of cardiac arrhythmia and is a major cause of ischemic stroke. Although direct oral anticoagulants have reduced stroke incidence, patients with a prior stroke remain at particularly high risk of recurrence, with annual rates reported at 7–10%. Identifying strategies to further lower this risk is therefore a major challenge in both neurology and cardiology.
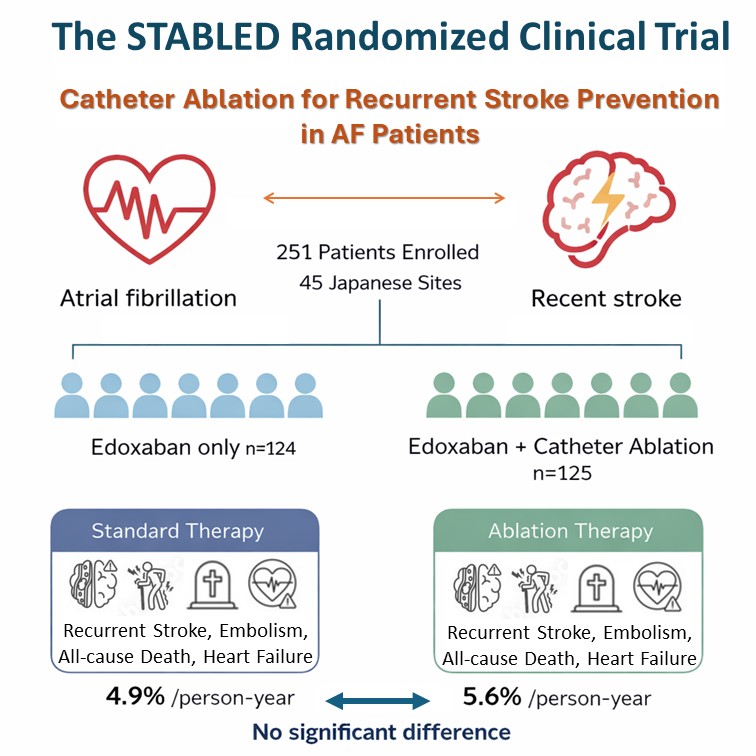
To address this clinical question, the Stroke Secondary Prevention With Catheter Ablation and Edoxaban (STABLED) randomized clinical trial enrolled 251 patients across 45 medical institutions throughout Japan. Participants were randomly assigned to receive standard therapy with the oral anticoagulant (edoxaban) alone or in combination with catheter ablation, an established procedure that aims to restore normal heart rhythm by eliminating abnormal electrical pathways.
After a median follow-up period of more than three years, researchers found no statistically significant difference in the primary composite outcome between the two groups. Event rates were 4.9% per person-year in the standard-therapy group and 5.6% per person-year in the ablation group.
The findings suggest that routine addition of catheter ablation to anticoagulant therapy may not provide a clear clinical advantage for secondary stroke prevention in this high-risk population. However, the investigators note that overall event rates were lower than expected, meaning the study may have been underpowered to detect smaller but clinically meaningful differences. Further research is needed to clarify whether advances in ablation technology or patient selection could improve outcomes.
The results were published online on March 2, 2026, in JAMA Neurology. The study was conducted through a nationwide collaboration involving multiple academic institutions and clinical partners across Japan, including Nippon Medical School and the University of Fukui, and the research funding was provided by Daiichi Sankyo Co, Ltd.
Trial Design and Primary Outcomes of the STABLED Randomized Clinical Trial
Image Caption:
Schematic overview of the nationwide STABLED randomized clinical trial comparing standard anticoagulant therapy alone with anticoagulant therapy plus catheter ablation in patients with atrial fibrillation who had recently experienced stroke. The rate of the primary composite outcome was similar between the two groups (4.9% vs 5.6% per person-year). These findings suggest that the routine addition of catheter ablation to anticoagulant therapy may not provide a clear additional benefit for preventing major cardiovascular events in this high-risk population.
Reference
| Authors |
Kazumi Kimura*#, Yasuhiro Nishiyama*, Yu-ki Iwasaki, Wataru Shimizu, Kazunori Toyoda, Yuki Sakamoto, Takehiro Katano, Teppei Yamamoto, Masataka Takeuchi, Kenta Kumagai, Kazuma Tsuto, Kaoru Sugi, Kengo Kusano, Masatoshi Koga, Seiji Okubo, Takahiro Sato, Hirotoshi Hamaguchi, Akihiro Yoshida, Ayako Kuriki, Kaoru Tanno, Kazuo Kitagawa, Nobuhisa Hagiwara, Hiroyuki Daida, Yasuyuki Iguchi, Shigeru Fujimoto, Susumu Miyamoto, Masayuki Fukuzawa, Masako Sugimoto, Atsushi Takita, Toshiaki Otsuka, Ken Okumura (*contributed equally, # corresponding author) |
| Title of original paper |
Catheter Ablation and Oral Anticoagulation for Secondary Stroke Prevention in Atrial Fibrillation: The STABLED Randomized Clinical Trial |
| Journal | JAMA Neurology |
| DOI | 10.1001/jamaneurol.2026.0155 |